GLASGOW COLORECTAL CENTRE
Scotland’s Best Private Colorectal Surgery & Colonoscopy Clinic
info@colorectalcentre.co.uk
If you have any questions, call Catherine on 0735 506 6597

© Glasgow Colorectal Centre. All Rights Reserved

Any questions? Call Catherine on 0735 506 6597
Info@colorectalcentre.co.uk
What are piles / haemorrhoids and what causes them?
Haemorrhoids (hemorrhoids USA) are swellings that can occur in the anus (also known as the anal canal or back passage). There is a network of small veins (blood vessels) inside lining of the anus and lower rectum. These veins sometimes become wider and engorged with more blood than usual. These engorged veins and the overlying tissue may then form into one or more small swellings called haemorrhoids.
The exact reason why these changes occur and lead to haemorrhoids forming is not clear. Some haemorrhoids seem to develop for no apparent reason. However, it is thought that the pressure in and around the anus can be a major factor in many cases. It is thought that an increase in pressure, in and around the anus may lead to the development of haemorrhoids.
About half the people in the UK develop one or more haemorrhoids at some stage. Certain situations increase the chance of haemorrhoids developing:
- Constipation, passing large stools (faeces), and straining at the toilet. These increase the pressure in and around the veins in the anus and seem to be a common reason for haemorrhoids to develop.
- Pregnancy. Haemorrhoids are common during pregnancy. This is probably due to pressure effects of the baby lying above the rectum and anus, and the affect that the change in hormones during pregnancy can have on the veins.
- Ageing. The tissues in the lining of the anus may become less supportive as we get older.
- Hereditary factors. Some people may inherit a weakness of the wall of the veins in the anal region.
What are the symptoms of piles / haemorrhoids?
Symptoms can vary from one person to the next and also from time to time in the same individual. Sometimes no symptoms may be present and a person may not realise that they have haemorrhoids (piles). Rectal bleeding is the most common symptom experienced. This often occurs after going to the toilet to pass stools (faeces). The blood is usually bright red and may be noticed on the toilet tissue, in the toilet pan or coating the stools.
A haemorrhoid can hang down (prolapse) and can be felt and seen outside the anus. Usually it can be pushed back up after you have been to the toilet. However, more severe piles remain permanently prolapsed and cannot be pushed back up inside.
Small internal piles are usually painless. Larger piles may cause a mucus discharge, some pain, irritation and itch. The discharge may irritate the skin around the back passage (anus). You may have a sense of fullness in the anus, or a feeling of not fully emptying your back passage when you go to the toilet.
A possible complication of piles that hang down is that they can strangulate (the blood supply to the haemorrhoid can be cut off). This can be intensely painful. Another possible complication is a blood clot (thrombosis) which can form within the haemorrhoid. This is uncommon, but again causes intense pain if it occurs. The pain usually peaks after 48-
What are the different types of piles / haemorrhoids?
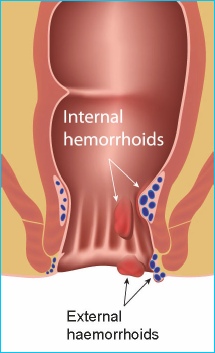
Internal haemorrhoids
These form in the back passage about 2-
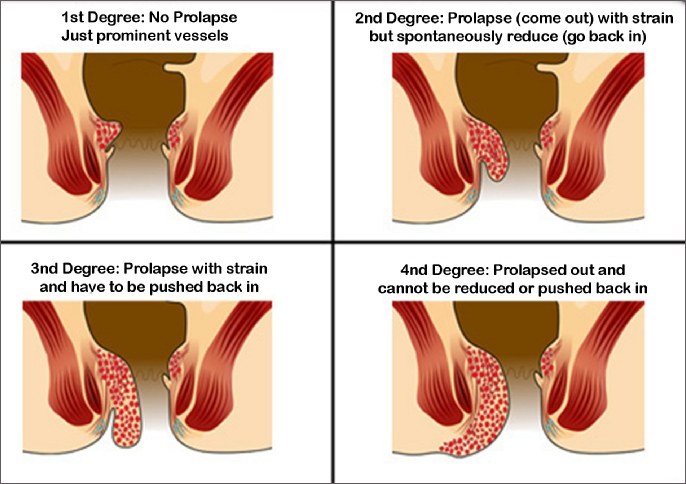
- Grade 1 are small swellings on the inside lining of the back passage. They cannot be seen or felt from outside the anus. Grade 1 haemorrhoids are common. In some people they enlarge further to grade 2 or more.
- Grade 2 are larger. They may be partly pushed out (prolapse) from the anus when you go to the toilet, but quickly 'spring back' inside again.
- Grade 3 hang out (prolapse) from the anus. You may feel one or more small soft small, soft lumps that hang from the anus. However, you can push them back inside the anus with a finger.
- Grade 4 permanently hang down from within the anus, and you cannot push them back inside. They sometimes become quite large.
Symptoms can vary. Small haemorrhoids are usually painless. The most common symptom is bleeding after going to the toilet. Larger haemorrhoids may cause a mucus discharge, some pain, irritation, and itch. The discharge may irritate the skin around the anus. You may have a sense of fullness in the anus, or a feeling of not fully emptying your rectum when you go to the toilet. Symptoms from haemorrhoids may be very similar to a number of other anorectal conditions so it is important not to simply assume that haemorrhoids are causing the problem. A colorectal surgeon/specialist will be able to confirm the diagnosis and also exclude any other problems.
A possible complication of haemorrhoids that hang down (grade 3-
External haemorrhoid (sometimes called a perianal haematoma)
This is less common than internal haemorrhoids. An external haemorrhoid is a small lump that develops on the outside edge of the anus. Many do not cause symptoms. However, if a blood clot forms in the haemorrhoid ('thrombosed external haemorrhoid') it can suddenly become very painful and need urgent treatment. The pain due to a thrombosed external haemorrhoid usually peaks after 48-
What is the best treatment for piles / haemorrhoids?
Avoid constipation and straining at the toilet
Keep the faeces (sometimes called stools or motions) soft, and don't strain on the toilet. You can do this by the following:
- Eat plenty of fibre such as fruit, vegetables, cereals, wholemeal bread, etc.
- Have lots to drink. Adults should aim to drink at least two litres (10-
12 cups) per day. You will pass much of the fluid as urine, but some is passed out in the gut and softens faeces. Most sorts of drink will do, but alcoholic drinks can be dehydrating and may not be so good. - Fibre supplements. If a high fibre diet is not helping, you can take bran or other fibre supplements (bulking agents') such as Ispagula (Fybogel ™), methyl cellulose, or Sterculia. You can buy these at pharmacies or get them on prescription. Methyl cellulose also helps to soften faeces directly which makes them easier to pass.
- Avoid painkillers that contain codeine such as co-
codamol, as they are a common cause of constipation. - Going to the toilet. Go to the toilet as soon as possible after feeling the need. Some people suppress this feeling and plan to go to the toilet later. This may result in bigger and harder faeces forming which are then more difficult to pass. Do not strain on the toilet. Haemorrhoids may cause a feeling of 'fullness' in the rectum and it is tempting to strain at the end to try and empty the rectum further. Resist this. Do not spend too long on the toilet which may encourage you to strain. (For example, do view sitting on the toilet as ‘quality time’ and avoid reading, contemplating life etc)
The above measures will often ease symptoms such as bleeding and discomfort. It may be all that you need to treat small and non-
Ointments, creams, and suppositories
Various preparations and brands are commonly used. They do not 'cure' haemorrhoids. However, they may ease symptoms such as discomfort and itch.
- A bland soothing cream, ointment, or suppository may ease discomfort. Several brands are available without a prescription. Ask a pharmacist to advise. Follow the instructions on the packet on how to use.
- One that contains an anaesthetic may ease pain better. You should only use one of these for short periods at a time (5-
7 days). If you use it for longer, the anaesthetic may irritate or sensitise the skin around the anus. A pharmacist can advise. - One that contains a steroid may be advised by a doctor if there is a lot of inflammation around the haemorrhoids. Steroids reduce inflammation and may help to reduce any swelling around a haemorrhoid. This may help to ease itch and pain. You should not normally use a steroid cream or ointment for longer than one week at a time.
- Very painful prolapsed haemorrhoids are uncommon. The pain may be eased by an ice pack pressed on for 15-
30 minutes. Strong painkillers may be needed. - Haemorrhoids of pregnancy usually settle after the birth of the child. Treatment is similar to the above.
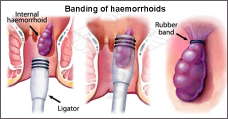
Banding treatment
Banding is a common treatment for grade 2 and 3 haemorrhoids. It may also be done to treat grade 1 haemorrhoids which have not settled with the measures described above (such as an increase in fibre, etc.).
This procedure is usually performed by a colorectal surgeon, either in the outpatient clinic or at the end of a flexible sigmoidoscopy or colonoscopy (these investigations are often performed on patients with bleeding from haemorrhoids in order to ensure that there is no other problem in the colon that might also account for bleeding).
The haemorrhoid is grasped by the surgeon with forceps or a suction device. A very small rubber band is then placed at the base of the haemorrhoid. This cuts off the blood supply to the haemorrhoid which then shrivels up and drops off after a few days. The tissue at the base of the haemorrhoid heals with scar tissue.
Banding of internal haemorrhoids is usually painless as the base of the haemorrhoid originates above the anal opening -
In about 8 in 10 cases, the haemorrhoids are 'cured' by this technique. In about 2 in 10 cases, the haemorrhoids recur at some stage. (However, you can have a further banding treatment if this occurs.) Banding does not work in a small number of cases. Haemorrhoids are less likely to recur after banding if you do not become constipated and do not strain on the toilet.
A small number of people have complications following banding such as bleeding, urinary problems, or infection or ulcers forming at the site of a treated haemorrhoid.
Injection sclerotherapy and other treatments
Phenol in oil is injected into the tissues at the base of the haemorrhoids. This causes a fibrotic (scarring) reaction which obliterates the blood vessels going to the haemorrhoids. The haemorrhoids then 'die' and drop off similar to after banding. However, this procedure is less widely used than banding because the success rate is not as good.
Various methods that use heat to 'destroy' the haemorrhoids. There are various ways this can be done and include: infrared coagulation; photocoagulation; diathermy; electrotherapy. However, these procedures are less widely used than banding because their success rate is not as good.
What are the surgery options to treat haemorrhoids?
Banding (described above) is perhaps the most common procedure done to treat haemorrhoids. However, a variety of other surgical procedures are sometimes used. Some surgeons prefer one procedure over another. Your surgeon will advise of the pros and cons of the different procedures. For example, although each procedure is usually successful, as with any surgical procedure, there is some risk that complications or problems may occur during, or following, the procedure. The more commonly done procedures include the following:
Haemorrhoidectomy (the traditional operation)
An operation to cut away the haemorrhoid(s) is an option to treat grade 4 haemorrhoids, and for grade 2 and 3 haemorrhoids not successfully treated by banding or other methods. The operation is done under general anaesthetic and is usually successful. However, it can be quite painful in the days following the operation.
Stapled haemorrhoidectomy
Although the name of this procedure implies that the haemorrhoids are removed (cut out), this is not so. What happens in this procedure is a circular stapling 'gun' is used to cut out a circular section of the lining of the anal canal above the haemorrhoids. This has an effect of pulling the haemorrhoids back up the anal canal. It also has an effect of reducing the blood supply to the haemorrhoids which shrink as a consequence. Because the 'cutting' is actually above the haemorrhoids, it is usually a less painful procedure than the traditional operation to remove the haemorrhoids.
Haemorrhoidal artery ligation (THD procedure / HALO Procedure)
In this procedure, a small proctoscope with a tiny embedded ultrasound, is used to identify the precise location of the small arteries that supply blood to the haemorrhoids. These arteries supply the haemorrhoidal tissue from the rectum. The proctoscope therefore allows the surgeon to accurately place a stitch in the lower rectum/upper anal cancel which reduced the blood supply to the haemorrhoid, causing them to shrink. If the haemorrhoids prolapse down, the surgeon can also place a stitch to “lift” up the loose tissue. The is also called an “anopexy”. This means that the surgeon can treat both the bleeding and also haemorrhoid prolapse without having to remove any tissue. As a consequence, it tends to be much less painful and is associated with a much faster recovery.
The THD procedure for haemorrhoids has therefore received a lot of national publicity and is gaining in popularity as the best treatment option after simple measures such a a change in diet and banding.
The THD procedure and the HALO procedure are almost identical in concept. The different names are derived from the fact that two different companies make equipment to perform the procedure and each has come up with their own name/abbreviation to differentiate it form the competition. The terms THD stands for “Transanal Haemorrhoidal Devascularization”, whereas the word HALO stands for “Haemorrhoidal Artery Ligation Operation”.
Strangulated or thrombosed piles
Very painful strangulated or thrombosed piles are uncommon. The pain may be eased by an ice pack (wrapped in a cloth) pressed on for 15-
What haemorrhoid treatments are available at the Glasgow Colorectal Centre?
It is important to undergo a complete assessment to confirm that the problem is indeed related to haemorrhoids and that there is not another cause for concern in the colon/bowel. Depending on the individuals age and any other anorectal symptoms, a colonoscopy may be advised in order to ensure the rest of the colon and rectum is healthy. If haemorrhoids are confirmed to be the main problem, all of the treatments described in this section are available and performed the colorectal surgeons at the Glasgow Colorectal Centre.
All of the above said, when considering treatments for patients who do not respond to more simple treatment measures such a change in diet, avoidance of staining and banding of haemorrhoids, we have found such good results with the THD procedure for haemorrhoids that we now tend to favour this procedure over other more invasive procedures such as haemorrhoidectomy.
Where can I get more information on treatment for piles / haemorrhoids?
There is a lot of information online regarding treating piles. Some of the better sites are listed below. In addition, we have separate web page on this website that gives more detailed information on the THD procedure for haemorrhoids. We also have an additional news item from the National Institute for Health and Care Excellence (NICE) that discusses the use of Haemorrhoidal Artery Ligation (THD procedure or HALO)
www.nhs.uk/Conditions/Haemorrhoids
NHS website proving information on haemorrhoids and treatments
Industry website providing information on anorectal conditions and the THD procedure for haemorrhoids
http://publications.nice.org.uk/haemorrhoidal-
NICE guidance on using Haemorrhoidal artery ligation for treating haemorrhoids



If you have any further questions about haemorrhoids or other colorectal issues, your own GP is often the best first port of call.
If appropriate, they will be able to arrange a referral to a colorectal specialist centre such as the Glasgow Colorectal Centre.
Haemorrhoids - Piles
Symptoms, treatment & surgery options
Haemorrhoids (piles) are swellings that contain enlarged and swollen blood vessels in the anus and lower rectum (back passage). Haemorrhoids are a common problem affecting up to 50% of adults at some point in their life. Symptoms range from temporary and mild, to persistent and painful. In many cases, haemorrhoids are small and symptoms settle down without treatment. If required, treatment is usually effective.