GLASGOW COLORECTAL CENTRE
Scotland’s Best Private Colorectal Surgery & Colonoscopy Clinic
info@colorectalcentre.co.uk
If you have any questions, call Catherine on 0735 506 6597

© Glasgow Colorectal Centre. All Rights Reserved

Any questions? Call Catherine on 0735 506 6597
Info@colorectalcentre.co.uk

What is bowel cancer?
Bowel cancer is a cancer of the colon or rectum. It is sometimes called colorectal cancer, colon cancer, rectal cancer or cancer of the large intestine. It is the third commonest cancer in the UK. (In contrast, cancer of the small intestine is rare.) Bowel cancer can affect any part of the colon or rectum. However, it most commonly develops in the lower part of the descending colon, the sigmoid colon, or rectum.
Bowel cancer usually develops from a polyp which has formed on the lining of the colon or rectum (see below). Sometimes bowel cancer begins from a cell within the lining of the colon or rectum which becomes cancerous. Some rare types of cancer arise from various other cells in the wall of the colon or rectum e.g. carcinoid tumours, GI stromal tumours (GIST), lymphoma and sarcomas)
As the cancer cells multiply they form a tumour. The tumour invades deeper into the wall of the colon or rectum. Some cells may break off into the lymph channels or bloodstream. The cancer may then metastasise (spread) to lymph nodes nearby or to other areas of the body, most commonly the liver and lungs.
What are the symptoms of bowel cancer?
The development of a bowel cancer from a polyp may take several years. When a colorectal cancer first develops and is small it usually causes no symptoms. As it grows, bowel cancer symptoms may develop. These can vary, depending on the site of the tumour. The most common anorectal symptoms to first develop are:
- Rectal bleeding, due to bleeding form the tumour. You may see blood mixed up with your faeces (stools or motions). Sometimes the blood can make the faeces turn a very dark colour. The bleeding is not usually severe and in many cases the bleeding is not noticed as it is just a small 'trickle' which is mixed with the faeces. However, small amounts of bleeding that occur regularly can lead to anaemia which can make you tired, pale and a decreased ability to work and exercise.
- Passing mucus with the faeces.
- A change in bowel habit from your usual bowel habit. This means you may pass faeces more or less often than usual causing bouts of diarrhoea or constipation.
- A feeling of not fully emptying the rectum after passing faeces. This feeling painful. Alternatively some patients with cancers low in the rectum may complain of a repeated painful, ineffective desire to want to move their bowel (called tenesmus)
- Abdominal pain/cramp
As the tumour grows in the colon or rectum, symptoms of the bowel cancer may become worse and can include:
- The same symptoms as above, but more severe.
- Feeling generally unwell/tired (feeling of malaise)
- Weight loss
- If the cancer becomes very large, it can cause a blockage (obstruction) of the colon. This causes severe abdominal pain and other symptoms such as vomiting.
- Sometimes the cancer makes a hole in the wall of the colon or rectum (perforation). If this occurs the faeces can leak into the abdomen. This causes severe pain.
If the cancer spreads to other parts of the body, various other symptoms can develop. The symptoms depend on where it has spread to. It is important to remember that all the the symptoms mentioned here can also occurs with other benign conditions. However, it is usually not possible not possible to be certain about what is causing these symptoms without undergoing a special test on the bowel. The most commonly performed test is a colonoscopy which is usually able to confirm or exclude a bowel cancer.
How does bowel cancer start?
Throughout our lives, the lining of the bowel constantly renews itself. This lining contains many millions of tiny cells which grow, serve their purpose and then new cells take their place. Each one of these millions of cells contains genes which give instructions to the cell on how to behave. When genes behave in a faulty manner, this can cause the cells to grow too quickly which eventually leads to the formation of a growth that is known as a polyp. This is the first step on the road towards cancer.
How do polyps cause bowel cancer?
A polyp, or more strictly a particular type of polyp called an adenoma, starts as a tiny bump on the inside of the bowel (colon or rectum). Most bowel polyps develop in older people. About 1 in 4 people over the age of 50 develop at least one bowel polyp.
At first, the genes give instructions for the polyp to grow in an orderly manner. Some polyps remain very small throughout their lives while others grow slowly larger. At this stage, the lump is still benign. Most polyps remain benign throughout life but about one in ten will turn into a cancer. Broadly speaking, the larger a polyp, the more likely it is to become cancerous -
How and why are bowel (colon) polyps treated?
Most polyps never develop into cancer. However, a small proportion of colon and rectal polyps may develop sinister or precancerous changes over time. Ultimately, some polyps develop into actual bowel cancers. In fact we believe that almost all cancers ultimately developed from small benign polyps. However it takes anything from 5 -
Most bowel polyps can be removed at the time of first detection during the colonoscopy or flexible sigmoidoscopy. Very large polyps or patients who are found to have multiple polyps may require more that one procedure to remove them all.
Some doctors have developed special skills in removing large polyps using the colonoscope and if a large polyp is detected, the colonoscopist who performed your procedure may decide to refer you on to a colorectal specialist who has developed these skills to remove large polyps with the colonoscope (therapeutic colonoscopy). Occasionally, it is not possible to remove a very large polyp with a colonoscope and surgery may be recommended. It is important to remember that
Most polyps do not contain cancer cells. However, removing the polyp prevents the risk that it may become cancerous sometime in the future.
Some polyps may already contain cancer cells at the time of removal. If these cells are confined to within the polyp then the removal of the polyp is curative. If the cells look as if they had begun to spread to the wall of the colon or rectum then an operation may be needed to remove that section of colon or rectum.
How common is bowel cancer?
Each year 35,000 people in Britain (just under 4,000 in Scotland) are diagnosed with bowel cancer (colorectal cancer or cancer of the colon and rectum). This makes it one of the commonest cancers. Unlike some malignant tumours, bowel cancer can often be cured by surgery and new treatments are being introduced to make survival even more likely. The earlier the bowel cancer is diagnosed, the greater the likelihood of cure.

Is there anything I can do to protect me from bowel cancer?
A diet rich in fresh vegetables and fruit, and low in red meat seems to help protect against bowel cancer. A high calcium intake may be protective as may be the regular ingestion of some anti-
The bowel cancer screening test is designed to identify individuals who polyps (and also cancers) at an early stage before they are causing symptoms. By identifying and removing pre-
There is increasing evidence that aspirin may reduce the risk of getting bowel cancer if taken for a sustained period of time. However, you should discuss this with your doctor rather than just starting this drug which can have side-
Does early diagnosis of bowel cancer make a difference?
Achieving a complete cure of bowel cancer depends on detecting it early on. The larger the growth and the more deeply and widely it has spread, the less likely it is to be curable. If people wait too long before reporting symptoms, the opportunity to remove the cancer completely may be lost. An early diagnosis can also be made in the absence of symptoms by the use of bowel cancer screening.
Aren’t the symptoms of bowel cancer similar to those of irritable bowel syndrome?
Yes they are. Symptoms of constipation and diarrhoea frequently occur with irritable bowel syndrome (IBS) and this can sometimes cause difficulty in making a diagnosis. A prolonged change in bowel habit lasting more than two or three months should always be investigated, and rectal bleeding is not a symptom of irritable bowel syndrome.
How is bowel cancer diagnosed?
Sometimes, the doctor will be able to detect a lump in the abdomen or on rectal examination but usually special tests are needed. The most commonly used are:
Flexible sigmoidoscopy. This is a telescope test that examines the lower one third or so of the lower bowel . It is normally performed after an enema. Most commonly it is performed without sedation although usually, you may be given a choice of sedation or no sedation.
Colonoscopy, is similar to a flexible sigmoidoscopy although the aim is to assess the whole of the lower bowel (all the colon and rectum). It therefore laxatives to clear out the bowel. These are usually taken the day before the procedure. The procedure is usually performed under “conscious sedation” which means light sedation. Many patients now opt no sedation .
CT colonoscopy or CT pneumocolon also involves taking bowl preparation is a relative newcomer. It involves a CT scan which is performed after a tube is placed in the anus to fill the colon with air. It has the advantage of being less uncomfortable than a colonoscopy (hence no sedation is given). However, it may not be as accurate as colonoscopy and of course, it is not possible to either biopsy or take off any polyps if these are seen. If this happens, it is may then be necessary to also have a colonoscopy.
Barium enema x-
Biopsy - to confirm the diagnosis
Both flexible sigmoidoscopy and colonoscopy have the advantage that a small sample or biopsy can be taken form an abnormal area. This can then be examined under the microscope to look for abnormal cells. If you have a colonoscopy or sigmoidoscopy, the doctor or nurse can take a biopsy of any abnormal tissue. This is done by passing a thin grabbing instrument down a side channel of the colonoscope or sigmoidoscope. It can take up to two weeks for the result of a biopsy.
Assessing the extent and spread
If it is confirmed that you have bowel cancer, further tests may be necessary to make sure that the cancer has not spread beyond the bowel. For example, blood tests and a CT scan of the chest and abdomen are performed in most patients. Additional scans may be necessary depending on the site of the cancer and also on the results of the first scans e.g. an MRI scan is frequently done in patients with rectal cancer or to look in more detail at the liver if the CT scan show any cause for concern. A PET-
- How much the tumour in the colon or rectum has grown, and whether it has grown partially or fully through the wall of the colon or rectum.
- Whether the cancer has spread to local lymph nodes.
- Whether the cancer has spread to other areas of the body (metastasised).
By finding out the stage of the cancer, it is possible for your medical team to advise on the best treatment options. It also gives a reasonable indication of outlook (prognosis). For colorectal cancer, it may not be possible to give an accurate staging until after an operation to remove the tumour.
Not only will the size of the primary tumour be assessed as fully as possible but your specialist will also want to know if there is any sign of secondary spread. Armed with all the relevant information they have gathered about the cancer, your specialists will decide how best to advise you on the most appropriate treatment.
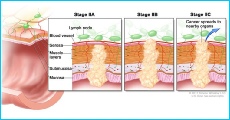
What are the stages of bowel cancer?
Worldwide, the TNM staging system is the most commonly used staging system. In this system, the depth of the tumour (T part), presence of absence of spread to the lymph glands or nodes (N part) and the presence or absence of distant spread or metastases (M part) is assessed in order to give a stage ranging from Stage 1 (earliest stage) to Stage 4 (most advanced stage). Detailed information on this staging system is available here.
Within the UK and Ireland, although the TNM staging is widely used, the Dukes’ classification is also used. This is shown here
- Duke Stage A: the cancer is confined to the inner lining of the colon or rectum.
- Duke Stage B: the cancer has grown into he muscle layer in the wall of the colon or rectum, but not beyond.
- Duke Stage C: the cancer has spread to at least one lymph node near to the colon or rectum.
- Duke Stage D: the cancer has spread to other parts of the body ('metastases' or secondary tumours). The most common site for colorectal cancer to spread to is the liver. Other places include the lungs, brain and bone.
How is bowel cancer treated?
Treatment often involves a number of different options that may be considered either on their own, or on occasion one treatment is followed by a different kind of treatment. Surgery forms the mainstay of treatment and is often combined with chemotherapy and occasionally radiotherapy. The treatment plan is specifically designed for each patient as a number of different factors need to be taken into consideration including the location of the tumour (e.g. radiotherapy is rarely used in colon cancers but frequently used to complement surgery in rectal cancers), the stage of the cancer, (how large the cancer is and whether it has spread) and the general health of the patient. Finally and perhaps most importantly, the patients wishes and goals for therapy play a pivotal role in deciding on a treatment plan.
Patients with a new diagnosis of bowel cancer should have a full discussion with a specialist who knows their case. They will be able to give the pros and cons, likely success rate, possible side effects and other details about the various possible treatment options for their type of cancer.
In the United Kingdom, the management of patients with a diagnosis of cancer is guided by a multidisciplinary team (MDT). The MDT consists of a number of specialist who deal with each specific cancer type. The team who deal with bowel cancer will usually include the following members
- Surgeons
- Oncologist (who give chemotherapy and radiotherapy)
- Pathologists (doctors who diagnose the cancer by examining samples of tissue under a microscope)
- Radiologists (doctor who specialise in interpreting and reporting the results of the various scan)
- Specialist nurses
- Palliative care doctors and nurses (who deal with symptoms of cancer)
Almost all new cases of bowel cancer are discussed at the local MDT for colorectal cancer. Each persons specialist will discuss their treatment plan and the aims of treatment. The aims of treatment will vary for each individual and also may vary over time, depending on the results of new scans etc.
Treatment may aim to cure the cancer. Many colorectal cancers can be cured, particularly if they are treated in the early stages of the disease. (Doctors tend to use the word 'remission' rather than the word 'cured'. Remission means there is no evidence of cancer following treatment. If you are 'in remission', you may be cured. However, in some cases a cancer may come back months or even years later. This is why doctors are reluctant to use the word cured.)
Treatment may aim to control the cancer. If a cure is not realistic, with treatment it is often possible limit the growth or spread of the cancer so that it progresses less rapidly. This may keep you free of symptoms for some time.
Treatment may aim to ease symptoms. If a cure is not possible, treatments may be used to reduce the size of a cancer which may ease symptoms such as pain. If a cancer is advanced then you may require treatments such as nutritional supplements, painkillers or other techniques to help keep you free of pain and any other symptoms.
Surgery
It is often possible to surgically remove the primary tumour. Removing the tumour may be curative if the cancer is in an early stage. Surgery is usually designed to remove both the cancer and to also include the nearby lymph nodes. The area of bowel that contains the cancer is then removed. It is usually possible to join the two ends of the bowel back together (anastomosed together).
In certain circumstances, it may be necessary to fashion a stoma (colostomy or ileostomy). A stoma means that the end of the bowel is brought out through an opening in the abdominal wall and the bowel content (faeces) comes out onto the abdomen, rather than out through the anus (or back passage). The faeces (poo) is collected into a special disposable bag or pouch that is attached over the stoma. If a stoma is necessary, it may be temporary or permanent.
Sometimes a temporary stoma is made, upstream of the join that was made after the cancer has been removed. This is most commonly necessary after surgery for rectal cancer. The aim of the stoma is to divert the bowel content away from the healing join (anastomosis). The stoma is usually reversed with a second operation a few months later when the joined ends of the colon or rectum are well healed.
If the tumour is low down in the rectum, then the rectum and anus may need to be removed. A permanent stoma may then be necessary. Fortunately, modern surgical techniques mean that permanent stomas are required much less frequently than in the past.
Even if the cancer is advanced and a cure is not possible, surgery may be required to relieve a blocked bowel and ease symptoms. However, increasingly, bowel blockages are being treated by inserting a thin metal tube (stent) through the blocked area to relieve the obstruction. Colonic stents are normally inserted in the x-
How is rectal cancer treated?
Unless they are very small and can be removed by a local operation, most cancers of the rectum need to be very carefully checked pre-
How is colon cancer treated?
Once a check has been made to see that there is no spread anywhere else most colon cancers are treated by surgery This usually involves removing the cancer together with the lymph glands alongside the blood vessels supplying that section of the bowel. In most cases, the two ends of the bowel are joined together again (anastomosis) but if the cancer has led to an emergency it may not be possible to join the bowel together straight away. Once the bowel cancer and surrounding tissue have been removed they are examined under the microscope in order to determine the precise stage of the cancer. If the cancer is confined to the bowel wall then surgical removal alone may be all that is needed. If there is any sign of spread to the local lymph glands a course of chemotherapy postoperatively may well be advised.
Does everybody with bowel cancer require chemotherapy and radiotherapy?
These treatments may be advised depending on the site and stage of the cancer. Chemotherapy is a treatment of cancer by using anti-
When chemotherapy or radiotherapy are used in addition to surgery it is known as 'adjuvant chemotherapy' or 'adjuvant radiotherapy'. For example, following surgery you may be given a course of chemotherapy or radiotherapy. This aims to kill any cancer cells which may have spread away from the primary tumour site. Sometimes, adjuvant chemotherapy or radiotherapy is given before surgery to shrink a tumour so that the operation to remove the tumour is easier for a surgeon to do and is more likely to be successful. This is then termed ‘neoadjuvant radiotherapy or neoadjuvant chemo-
What happens after surgery?
While you are recovering, the MDT team will meet to consider whether further treatment is advisable. Such decisions are based largely on the information about how advanced the primary cancer was. After the operation, the treatment options will be explained to you by your specialist and if there is a need for further treatment such as chemotherapy -

What is the prognosis (outlook) for bowel cancer?
The prognosis varies for each individual. There are a number of factors that affect prognosis but the Stage of the cancer is perhaps the most important. There has been a substantial improvement in the prognosis of people with colorectal cancer over the past decade. Without treatment, a colorectal cancer is likely to get larger and spread to other parts of the body. However, in many cases it grows slowly and may remain confined to the lining of the colon or rectum for some months before growing through the wall of the colon or rectum, or spreading. There is a good chance of a cure if bowel cancer is diagnosed and treated when the cancer at an early stage.
Figures published in 2009 from the National Cancer Intelligence Network showed that people diagnosed at an early stage (stage A) have more than a 9 in 10 chance of surviving the disease. At present, only about 1 in 7 people with colorectal cancer are diagnosed at stage A as the disease does not often cause symptoms at this early stage. However, patients diagnosed through the Bowel Cancer Screening programme tend to have cancers at an earlier stage.
If the cancer is diagnosed when it has grown through the wall of the colon or rectum, or spread to other parts of the body, there is less chance of a cure. However, treatment can often slow down the progression of the cancer.
The treatment of cancer is a developing area of medicine. New treatments continue to be developed and the information on outlook above is very general. Your specialist can give more accurate information about your particular outlook, and how well your type and stage of cancer is likely to respond to treatment.
What is advanced bowel cancer?
This is when the cancer has spread from the large bowel itself to other sites in the body. This may have already happened when the cancer is first diagnosed or may occur at a later date. The most common site for the cancer to spread is to the liver, although bowel cancer may also spread to other areas including the lungs, bone and the brain. Chemotherapy in this situation can be effective in controlling symptoms and prolonging life. Chemotherapy does not cure the disease and treatment is selected to provide a balance between the side effects and the benefits gained from treatment.

If I already had a bowel cancer, what can I do to stop it coming back?
A healthy life-
If I have been diagnosed with bowel cancer, what are the implications for my family?
If a person is young (40-
There are uncommon and inherited conditions including familial adenomatous polyposis (FAP) in which numerous polyps develop throughout the bowel and the cancer risk is greatly increased. The family of these patients has to be carefully screened.
What is bowel cancer screening?
Mass screening of the general population for bowel cancer has now started in the UK. Because polyps and cancers have a tendency to bleed small amounts (often so small that you do not see it ), one of the screening methods involves performing a special test on the faeces (poo) to see if it contains microscopic traces of bleed (Faecal Occult Blood (FOB) test). If this initial test is positive, then individuals with a positive FOB test are invited to go for a colonoscopy. The FOB screening test is now up and running throughout the UK. In Scotland, the FOB test is sent out every 2 years to the whole population aged 50 -
A second type of screening for bowel cancer is also undergoing evaluation. This involves inviting everyone between the ages of 55-
Both the FOB screening and flexible sigmoidoscopy screening appear to show that they identify more early cancers and also prevent cancers f the bowel from developing as the pre cancerous polyps can be detected and removed before they get a chance to develop into a cancer.
What cancer research is being performed into bowel cancer?
New surgical techniques (e.g. laparoscopic or keyhole surgery) are being used to reduce the size of the abdominal wound and allow and faster or enhanced recovery. Robotic surgery techniques are now also used in certain situation to try and get a more accurate removal of the bowel.
Chemotherapy has certainly been increasingly successful over the last few years as cancer research has led to the development of a number of new drugs which are now available. Aspirin-
Is it possible to undergo investigation and treatment for bowel cancer  at the Glasgow Colorectal Centre?
at the Glasgow Colorectal Centre?
Glasgow Colorectal Centre surgeons, Richard Molloy and Ahmed Alani are colorectal surgeons who specialise in diagnosing and treating bowel cancer. The Centre is based at BMI Ross Hall hospital which has state of the art Endoscopy suite with the latest high definition Pentax colonoscopes, modern up to date CT and MR scanners, a fully equipped theatre and high dependency and intensive care unit. They work closely with their oncology, pathology, radiology and anaesthetic team to provide a fully integrated package of care for patients with bowel cancer.
Where can I get further help and information on bowel cancer?
Bowel Cancer UK
7 Rickett Street, London, SW6 1RU
Tel: 08708 50 60 50 (Bowel Cancer Advisory Service) Web: www.bowelcanceruk.org.uk
Is dedicated to raising awareness, improving the quality of life of those affected and ultimately, reducing deaths from bowel cancer.
Beating Bowel Cancer
Harlequin House, 7 High Street, Teddington TW11 8EE
Tel: 08450 719 300 Tel (Nurse helpline): 08450 719 301 Web: www.beatingbowelcancer.org
A national charity working to raise awareness of symptoms, promote early diagnosis and encourage open access to treatment choice for those affected by bowel cancer.
Bowel Cancer Wales
Sherwood, Llandraw Woods, Maesycoed, Pontypridd R.C.T, CF37 1EX
Tel: 01443 408813 Web: www.bowelcancerwales.com
Aims to raise awareness of the disease and raise funds to research bowel cancer in Wales
Macmillan Cancer Support
Tel: 0808 800 1234 Web: www.cancerbacup.org.uk
They provide information and support to anyone affected by cancer.
Cancer Research UK
Web: www.cancerhelp.org.uk provides facts about cancer including treatment choices.
NHS Bowel Cancer Screening Programme
England -
Scotland -
Wales -
Northern Ireland -
NICE - National Institute for Health and Clinical Excellence
Web: www.nice.org.uk/guidance/index.jsp?action=byTopic&o=7174
This link takes you to various guidelines relating to colorectal cancer. Each guideline usually has a corresponding information for the public' to explain things in plain English.


If you have any further questions about bowel cancer or other colorectal issues, your own GP is often the best first port of call.
If appropriate, they will be able to arrange a referral to a colorectal specialist centre such as the Glasgow Colorectal Centre.
Bowel (Colorectal) Cancer
Symptoms, diagnosis and treatment of bowel cancer
Bowel or colorectal cancer (also called cancer of the colon or rectal cancer) is the third most common cancer in Scotland. Every year in Scotland, almost 4,000 people are diagnosed with the disease. Most cases occur in people over 50 years of age. Although bowel cancer is common, it is also very treatable if detected early. When bowel cancer is detected in it’s early stages, there’s more than a 90% chance of successful treatment. The sooner it’s caught, the easier it is to treat.